
Ideologically driven approach to SEND fails to help "neurodiverse" pupils
The PINS programme failed to have a measurable impact on pupil attainment, attendance, exclusions, or suspensions

The background to PINS
In recent years, policymakers have become extremely concerned about provision for pupils with Special Educational Needs and Disabilities (SEND). According to statistics published by the Department for Education (DfE), the number of children identified as having SEND, and the number qualifying for the most expensive provision (an EHC plan), have both been increasing at an ever-greater rate over the last ten years.
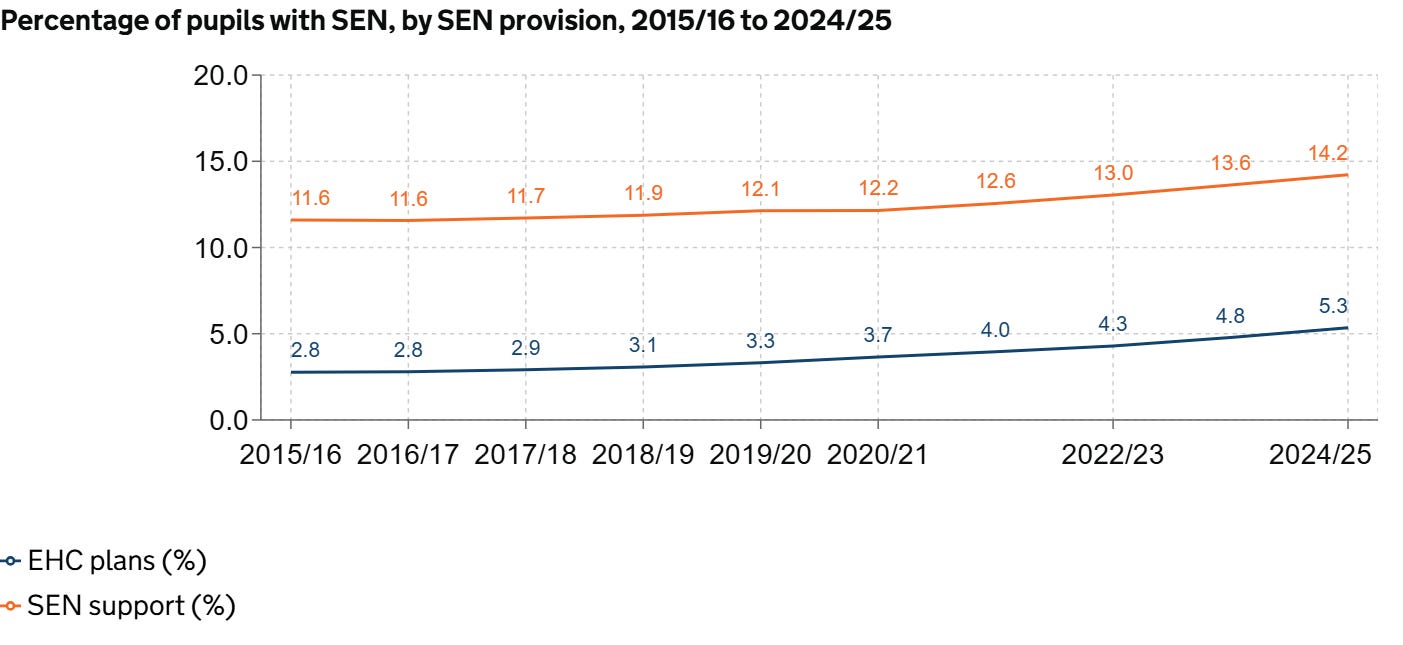
Underlying this are rises in specific types of need:
Autistic Spectrum Disorder: Increased from 100,801 in 2015/16 to 263,989 in 2024/25.
Speech, Language and Communication Needs: Grew from 225,245 to 396,025.
Social, Emotional and Mental Health: Rose from 194,691 to 350,534.
Schools, Multi-Academy Trusts and Local Authorities are crying out for help, and controversy rages over the causes of the increase. Is it a result of a genuine change in need (perhaps as a result of pandemic lockdowns)? Could it be an attempt to explain (or excuse) the more challenging behaviour seen in schools since COVID-19? Or does it have something to do with the way parents on social media boast in their bios about how “neurodivergent” (or, in some cases, “neuro-spicy”) their children are?
Could medical expertise solve the problem?
A big difficulty is that the procedures and systems used to identify children as SEND are neither rigorous nor evidence-based. A child’s label will differ depending on where they live, which school they attend, or how pushy (and well-resourced) their parents are. It would make sense to draw more heavily on the clinical expertise of the medical professions to inform the current system of arbitrary and bureaucratic identification of needs. Resources could also be saved by ensuring that provision was evidence-based (as in most medical research), rather than driven by fads and ideology (as in much education research).
Unfortunately, a recent collaboration by the DfE and NHS England has spectacularly failed to add scientific rigour to the system. It has also failed to help children in any measurable way.
According to the DfE website, Partnerships for Inclusion of Neurodiversity in Schools (PINS) is:
…a national programme that brings specialist health and education professionals and expert parent carers into mainstream primary schools to:
help shape whole-school special educational needs and disabilities (SEND) provision
provide early interventions at a school level
upskill school staff
support the strengthening of partnerships between schools and parent carers
What is “neurodiversity”?
The name alone should give us reason to worry. “Neurodiversity” is not a medical diagnosis;1 it’s a label that was coined by a sociologist and adopted by activists campaigning for the civil rights of people with autism, ADHD and other conditions. Which other conditions are included is not always clearly defined. Footnotes to the DfE web page I quoted earlier explain just how loosely this project relates to actual diagnosable categories of need:
[footnote 1] Neurodiversity is the concept that everyone’s brain is unique. It recognises the biological fact that we are all diverse – we all think, learn and act differently, and have different strengths. Neurodiversity recognises and celebrates the value that these different strengths can bring.
[footnote 2] Neurodivergent children may have a formal diagnosis such as autism, ADHD, dyslexia, etc. However, we recognise that many neurodivergent children do not have a formal diagnosis. Many of the approaches and interventions promoted through the PINS programme will be of benefit to all children, including those who may have other types of SEND, mental health needs or learning difficulties. Access to support provided through the PINS programme is not dependent on any formal diagnosis or assessment, and the list of conditions that may be supported is not exhaustive.
One executive headteacher involved in PINS describes neurodivergent conditions as ranging “from autism, ADHD and anxiety, to dyslexia, dyspraxia and more”, suggesting it covers both developmental disabilities and mental health issues. This is an umbrella term that covers children who have little in common. If anything, it is likely to encourage the proliferation of labelling, rather than challenge it.
So if PINS is not about bringing medical rigour to the identification of SEND, what does it provide?
Activism disguised as expertise
In practice, PINS seeks to provide training to schools which is more ideological than evidence-based.
[PINS] will support a shift away from the need for diagnosis and more intensive levels of support for individual pupils to focus instead on:
strengthening knowledge and skills
improving environments to better meet the needs of all children, but with a particular focus on neurodivergence2
It’s actually difficult to find much reference to the content of the training on the DfE website. Fortunately, some local authorities have shared the documentation from the scheme. Again, the lack of specificity is clear:
This project covers the full range of neurodiversity, and any training and support provided should cover a range of needs, including (but not limited to) ADHD, autism, neurodiversity and anxiety, dyslexia, dyspraxia, dysgraphia, dyscalculia, developmental language disorder, foetal alcohol syndrome, and other forms of developmental learning differences and needs (this list is not exhaustive). Being needs- rather than diagnosis-led, it also covers children without a formal diagnosis.
As for the content of the training, teachers whose careers stretch back to the disastrous “Inclusion” era of the 00s might find it very familiar. PINS aims “to sustainably create inclusive schools, including influencing teaching practices and curriculum development”.
The document tells us about the “Indicative content” of the scheme, which includes:
…Supporting staff to understand their own reactions to neurodiverse children and their behaviours, and the importance of double empathy.
…Experienced professional support for schools to review policies and procedures to increase inclusivity and support the implementation of child-centred planning
…Developing pupil voice opportunities within the school, including the voices of neurodiverse children, and exploring best practice in coproduction with pupils, including in the development of new policies and a more inclusive culture in school.
…Exploring common factors in the academic environment that can increase anxiety for neurodiverse children.
…Raising awareness of the impact that other factors such as trauma, attachment difficulties, and the existence of other co-occurring conditions e.g. anxiety, can have on the mental health of neurodiverse children.
Developing emotional resilience in staff when working with children with behaviour that challenges, including neurodiverse children.
…Developing a sense of “belonging” to, and engagement with, the school or setting amongst all pupils…
…Ensuring school leadership and policy addresses any reasonable adjustments that may be appropriate for neurodiverse children when managing behaviour that challenges.
Supporting schools to understand the functions of certain behaviour in neurodiverse children and considering strategies to support behaviours that challenge, ensuring they are person centred…
…Considering the use of highly motivating tasks as an approach to supporting children to engage neurodiverse children in education.
…supporting school staff to develop a toolkit of alternative approaches to teaching core skills, e.g. phonics and basic maths skills…
…Developing an understanding of a range of cognitive functions and learning styles…
…Developing staff understanding of good universal support for speech, language and communication skills. These include: …The opportunities that are planned for children to communicate – such as group work, talking partner activities and class discussions.
The extent to which this seems reasonable or fills you with dread might well depend on whether you have seen language like this in the past. For those of us who taught in the 2000s and saw similar words used to justify extreme dumbing-down and the tolerance of dangerous and disruptive behaviour, this seems like a massive step backwards. At the very least, this language suggests a lack of interest in keeping expectations high for those who struggle. It’s also a blow to advocates of evidence-based education. Who would expect to see the long-debunked concept of “learning styles” appearing in a DfE publication in 2025?
Another indicator that this is inspired more by activism than science is that some of the content reflects the identity politics era around 2020. “Indicative content” also includes:
…Exploring the difference between equality and equity.
…Looking at intersectionality, such as neurodiversity and race.
…Supporting schools to develop clear plans … celebrating neurodiversity and inclusion.
It makes sense to “celebrate” one’s identity, particularly when campaigning for greater recognition and acceptance. It makes no sense at all to celebrate suffering from anxiety or being unable to read. This made me wonder who was running this programme. I found that one local authority included details of their PINS team3, and I was somewhat shocked to see statements like this:
“I am a mother of a child who has a diagnosis of Autism, ADHD and Pica. As a result, I am passionate about raising awareness and understanding of Autism and neurodiversity.”
And also:
“I am neurodiverse and so have a passion for supporting neurodiverse children and young people to feel heard…”
These sound more like the social media bios of activists than what one expects from those charged with running an experimental medical/educational protocol affecting vulnerable children.
Perhaps the most worrying thing isn’t the educational ideology, or the political one; it’s the medical one. Cognitive Behavioural Therapy, one of the most evidence-based interventions for children with mental health needs, is disparaged.
Building awareness that talking therapies such as CBT may not be appropriate for many neurodiverse children with speech and language challenges including developmental language disorder and exploring alternative routes of therapeutic support.
It doesn’t say what these “alternative routes” are, but there is no end of charlatans out there offering crank therapies to schools and parents. From Attachment Therapy to Dyadic Developmental Psychotherapy, there’s no shortage of ways schools can waste money failing to help vulnerable children. It is well established that some psychotherapies can even be harmful. This is an extraordinarily irresponsible message to give to schools, even if it may have been intended to address genuine challenges with using talking therapies with uncommunicative children.4
So does indoctrinating teachers result in measurable gains for children?
Of course, it doesn’t. However, it looks like some serious effort has been made to obscure this.
The explanatory note, containing information for all school and academy trust staff taking part in the PINS Programme, had explained that:
DfE will commission a high-quality mixed method and multi-informant process and impact evaluation. The evaluation will run for 18 months between January 2024 and July 2025 in parallel with delivery and completion of the programme. The aim of this evaluation is to understand how PINS was implemented and to examine the impact of the programme on outcomes for neurodiverse children.
However, when the evaluation of the programme was published this week, it was labelled as an “interim” report and was stuffed with subjective content from surveys and anecdotal evidence. It was remarkably lacking in discussion of measurable outcomes. The first appendix lists the following among outcomes to be considered in evaluating PINS:
Reduction in suspensions and formal exclusion among neurodiverse pupils
Reduction in persistent absence and part-time timetables among neurodiverse pupils
Improved attainment of neurodiverse pupils
These have all now been classified as “long term”.5
How and why did this happen? It’s hard to tell. The aims of the original project were quite clear; they included the following objective: “Determine how and to what extent PINS improved child outcomes”. The redefining of a key objective as a “long term” aspiration is probably connected to the fact that, according to page 88, “the evaluation does not yet show measurable impacts on pupil outcomes”. In fact, it’s worse than that. Not only is there no measured improvement in pupil outcomes, but even “evidence of perceived [my emphasis] improvements in pupil outcomes is currently limited”.6 This would suggest that even the illusion of improvement has failed to take hold.
Unfortunately, the report argues that the anecdotal and survey evidence is sufficient to declare the programme a success. Inevitably, it claims that:
To increase the likelihood of implementing the PINS approach beyond the national programme, additional resources and/or more evidence of the scale and nature of the impact will be required.
This is a post hoc argument that is completely inconsistent with what was promised. PINS has failed to show a measurable impact in its first evaluation. This is to be expected, given its dubious content, and should be seen as grounds for abandoning it, not doubling down. Let’s hope that at least some key policymakers recognise this.
I should note that, when describing individuals, the term “neurodivergent” is often used. PINS refers to both “neurodiverse” and “neurodivergent” children (or pupils).
I won’t link because I’m obviously not interested in attacking individuals. I am just curious about the professionalism with which this project is being implemented.
Because I don’t discount these challenges, I would not object to medical specialists evaluating what therapy is appropriate for a particular child. Schools, however, should not be doing this.
It’s hard not to wonder when in the process this happened. In the main report, “long-term” is generally written with a hyphen. In the Appendix, it is written without the hyphen. Was it written at a different time? And if so, was it before or after it emerged that these outcomes showed no improvement?
Page 16.